
Reading about death and suicidality can be distressing. Please read this in a moment where you feel safest and ready to do so.
Pediatricians, child psychologists and psychiatrists, social workers and pediatric emergency teams know something that many people who care for children don’t: we are much busier during the school year. I’m a full-time emergency psychiatrist who works at a major children’s hospital, and often when children come in for a mental health crisis, one of the main stressors they discuss is school.
I’m sure most people assume I commonly prescribe medications as a physician, but one of my most common “prescriptions” is advocating for reducing school burden and load. In a 2013 American Psychological Association survey, 83 percent of adolescents stated that school was a cause or significant source of stress. In a 2017 survey of school leaders in the U.K., 82 percent reported increased mental health issues among primary school children during the time of national examinations. In studies in 2013 and 2015, scientists studying homework in the U.S. found that primary school children were averaging 30 minutes of such work per night, while high-performing secondary students were averaging more than three hours per night, at the cost of their physical health and schoolwork-life balance.
Whether we are talking about referrals to mental health programs for crisis, presentations to emergency departments for mental health issues, admissions to intensive care units for urgent treatment of suicide attempts or deaths by suicide, an association with school is clear. We are able to visualize this in a number of ways.
By using the Centers for Disease Control and Prevention’s Wonder database to find information on pediatric (17 years of age or younger) deaths by suicide, I have created a “heat map” of youth suicide, and a school-day association is plain to see. On weekdays and during school months, there is a significant elevation of suicide deaths in children.
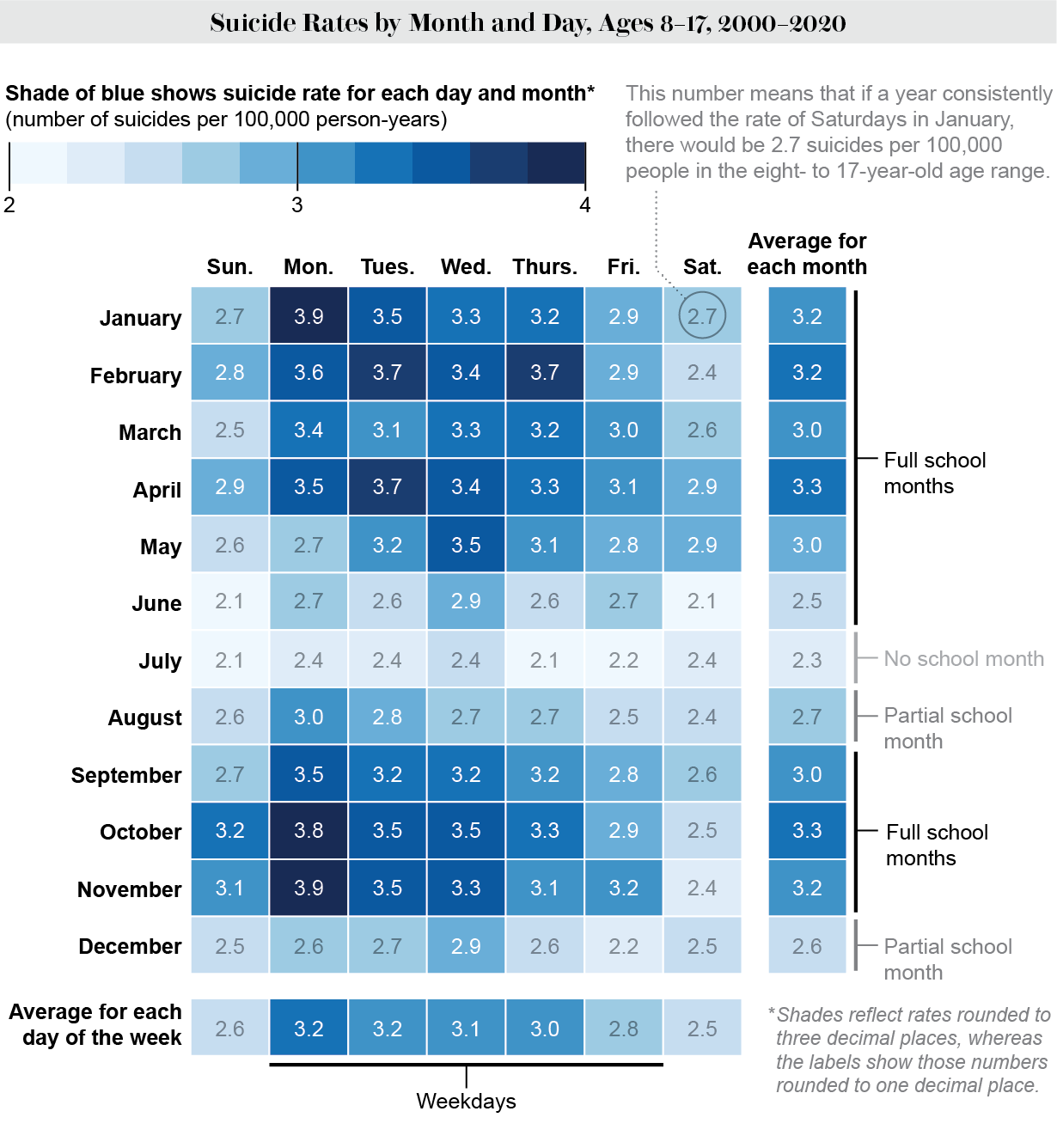
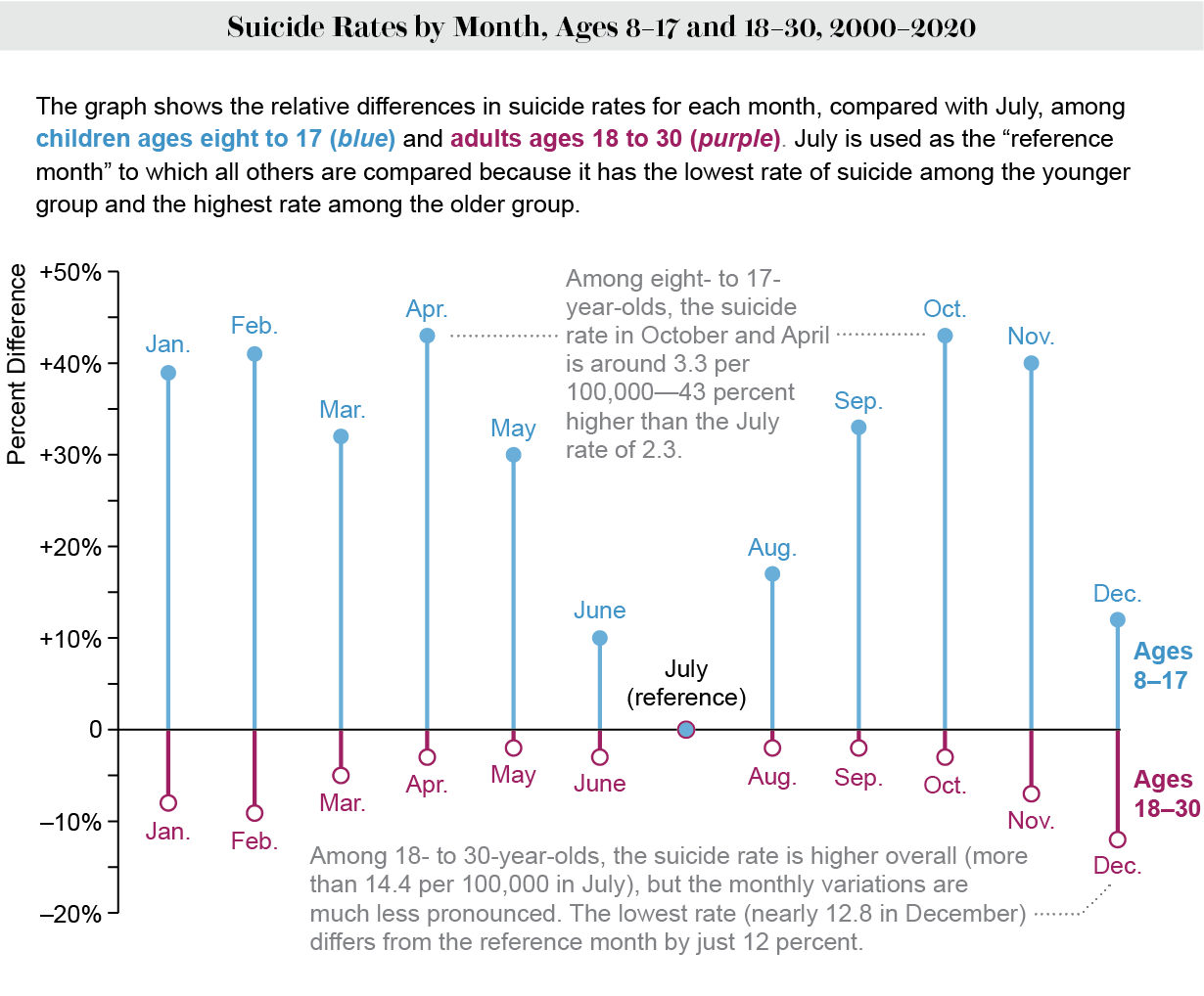
Looking at the monthly data, we can see that this elevation is not trivial: during school months, the increase in pediatric suicides ranges between 30 and 43 percent. This is in sharp contrast with adults, where we see suicide rates typically peak in summer months.
This situation has not improved over time: Compared with summer weekends, school-month weekdays from 2016 to 2019 show a pediatric suicide rate increase of 62 percent. The increase was 42% from 1999 to 2015.
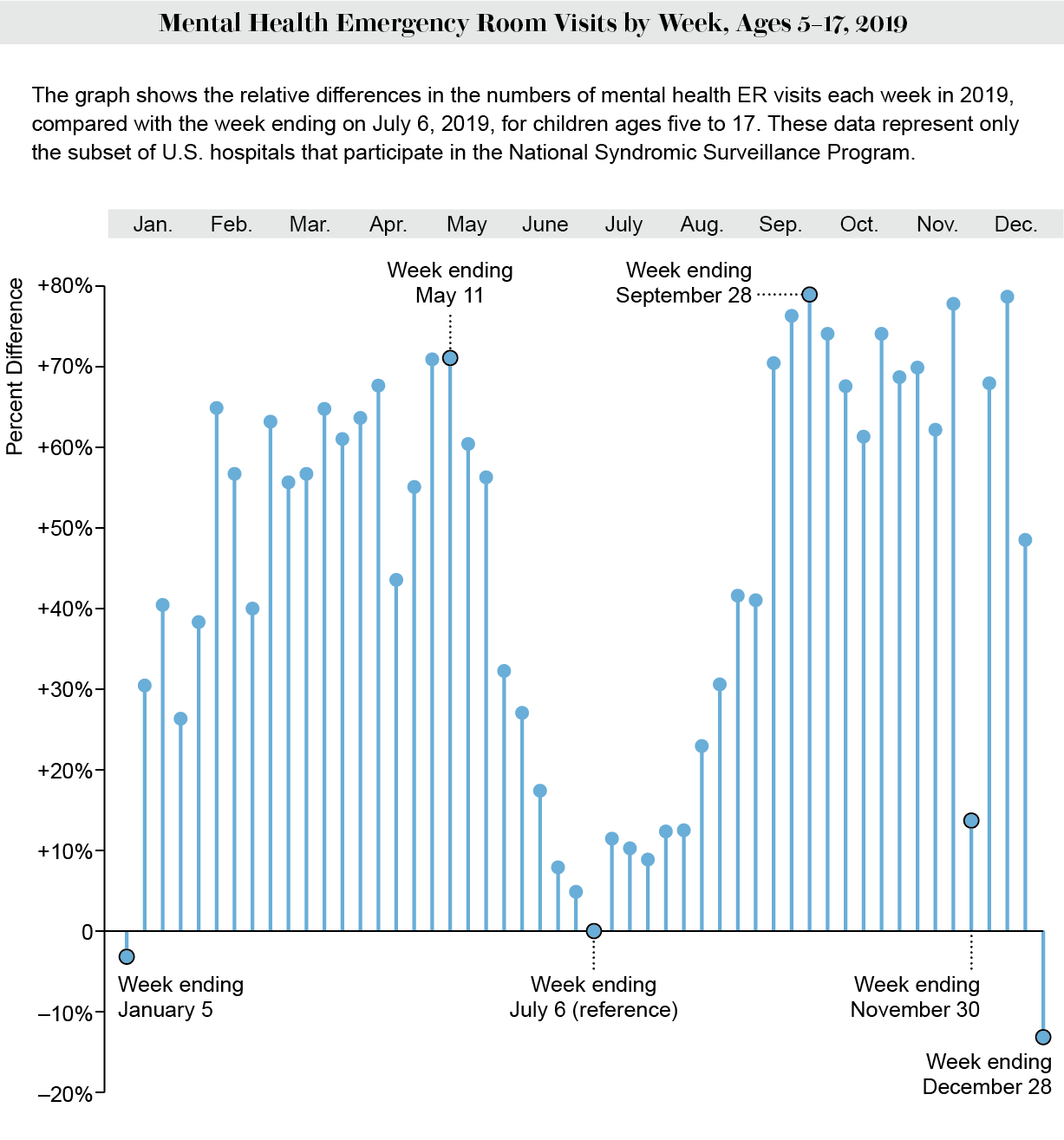
If we look at far more common events, such as emergency room visits for mental health conditions, we see a strikingly similar pattern. These data come from participating hospitals in a collection done by the CDC.
School comes with many things, good and bad. School can be wonderful, with learning experiences, social successes and a sense of connection to others. But it can also be incredibly stressful because of academic burden, bullying, health- and disability-related barriers, discrimination, lack of sleep and sometimes abuse. I often liken going to school to a child’s full-time job. The child has co-workers (classmates arranged by hierarchy), supervisors (teachers), bosses (administrators and principals) and overtime (homework). And they have very early work hours (most schools have hours that are very incompatible with children’s sleep patterns). Of course, work can be rewarding, but it’s also stressful.
Any time I present these data to teachers, parents, principals or school administrators, they are shocked. This should be common knowledge. Pediatric suicides and mental health crisis rates increase sharply when school is in and ease when school is out. This pattern is also found in other jurisdictions, such as Japan, Germany and Finland.
There are a number of ways to potentially mitigate this distress that I wish those responsible for our children’s education would explore. Some suggestions I’d put forth:
-
Reduce homework (preferably get rid of it). Some of the best educational science available shows that excessive homework is of limited benefit and in fact harms children’s health and well-being.
-
Add a mental health curriculum. We have developed incredible educational goals for math, reading, science and the arts. There should be a dedicated pathway for a much more universal and necessary learning: how to take care of yourself; how to look out for and help others; and how to improve both the detection and prevention of mental health crises.
-
Take bullying seriously and don’t just focus on the bullies. The bullied and bullies often come from similar backgrounds (histories of abuse, trauma, chaos, deprivation, parental detachment, though this certainly isn’t universally the case). But whereas the bullied tend to be internalizers, the bullies are more often externalizers. Bullies who were once victims of bullying have the highest risk of having psychiatric problems in the future.
-
Restore funding for playtime, music and art in school and de-emphasize academic overload. Children need relaxation, comfort, beauty, fun and play. Children who have opportunities to play and rest will learn more in their academics, and they will be able to sustain their development as they grow.
-
End “perfect attendance” awards and goals. While problematic truancy should be addressed, there is no less realistic notion for the rest of one’s life than the idea of “perfect attendance.” We should all, from time to time, recognize when we are at our limit and need a break. Children should be encouraged to report when they can do so and be supported.
-
Start school later. How many more decades of research do we need to show that children need more sleep and that adolescents do better in school when the day starts later? It’s time to make serious structural changes to the early-morning wake-up times.
-
Be nonjudgmental and respect children’s identity and identity formation. This is not a “woke” concept. This is a caring, compassionate concept that works for all children all the time.
-
Recognize and address child abuse within schools. There exist (and many readers may likely recall) teachers who are abusive, punitive and cruel. In one 2015 study, 44 percent of undergraduates recalled a time in K–12 school that they labeled as emotional abuse by a teacher. And in another study published in 2019, 3.4 percent of seventh- and eighth-grade students reported teachers bullied them.
Every year my colleagues in the emergency department brace for the coming mid-September wave, as every year our mental health crisis presentation volumes double and our days become much busier. Likely not coincidentally, in my jurisdiction, school starts in the second week of September.
In the new school year, if you are someone who works with school-age children, ask yourself what you could be doing to reduce pressure or improve quality of life for the children in your care. This would truly be suicide prevention.
IF YOU NEED HELP
If you or someone you know is struggling or having thoughts of suicide, help is available. Call or text the 988 Suicide & Crisis Lifeline at 988 or use the online Lifeline Chat. LGBTQ+ Americans can reach out to the Trevor Project by texting START to 678-678 or calling 1-866-488-7386.
This is an opinion and analysis article, and the views expressed by the author or authors are not necessarily those of Scientific American.
 Rights & Permissions
Rights & Permissions
